By the end of the 19th century, the discovery of x-rays had led to a revolution in Medicine. Doctors were now able to see inside the body without the use of invasive procedures. Radiology, or diagnostic imaging, that used x-rays as an imaging modality, came into existence. The decades that followed saw advances in leaps and bounds. New modalities for noninvasive diagnosis of disease were introduced into radiology: Ultrasound imaging, CT scan, MRI, PET, some less harmless than others. The imaging techniques that had started out requiring the manipulation of x-ray films, including the later developed newer hybrid systems, were now producing digitalized images, capable of being manipulated and enhanced in mind boggling ways by advances in signal processing and the continued improvement of image resolution.
The 2D image breakthroughs were joined by 3D imaging modalities in which several images could be taken and processed to create volume representations of tumors. Consequently, surgeons could make use of real time 3D image-guided surgical navigation systems, where tumors could be identified and located, tagged by radiopharmaceuticals, and then excised or ablated. Nonsurgical, or at the most, minimal invasive surgery, diagnosis and therapy became a useful tool for the interventional radiologists. This tool, radiosurgery, or stereotactic radiosurgery, which involved no actual incisions, used high-energy x-rays, gamma rays or proton beams, that were directed to alter or destroy the target tumor’s DNA, resulting in its size reduction over time.
Unfortunately, 3D technologies were characterized by image distortions, introduced by the movement of structures during breathing, for example. This affected the precision of volumes and locations of target tumors. However, the introduction of time, a required variable for motion characterization, in this 3D signal analysis, led to the creation of volume-time 4D medical imaging and radiation therapy which have resulted in even better-quality images, and correspondingly, better diagnoses and treatment.
However, radiology is not just about the new technologies at the disposal of the radiologists.
The practice of medicine is akin to a team sport. Teams of individuals work together for the greater good (better health care) of the patient and by extension of the society. In teams, however, some members feature more prominently than others, or are more visible to the public because of the peculiarities of their role. It behooves us not to determine value or importance based on visibility. For the patient, the radiologist is a phantom, hardly seen, or if seen, not easily identifiable, but for the gamut of medical and surgical specialists or even the generalists, a quintessential team member.
Dark rooms, humming of fans in black boxes, a human, wearing a white coat, seated for hours at a time, with eyes glued to one screen and then another, and sporadic chatter are the commonly reported scenes of passersby. The life of the radiologist is so much more. Early awakening, holding lectures, presenting cases and new advancements to other radiologists, radiologist residents, other doctors, or even technicians, at conferences or symposiums, nationally and internationally, receiving consultations, internally and externally, studying and analyzing images, reading up on new literature, creating radiation treatment plans, writing impressions and diagnoses, authoring or co-authoring articles, or even physically examining patients, are some of the basic expectations of these professionals.
The life of the radiologist is inextricably embedded in the tapestry of civilized society. They have families, friends, hairdressers, barbers, bankers. Gardeners, housekeepers, au pairs or nannies, or drivers might be their employees. They shop at the supermarkets and clothing stores, eat at restaurants, visit amusement parks, go to a basketball game, stay in hotels, take their cars and trucks to the mechanic, buy gas, pay for utilities, and purchase houses, just as other humans do. Any trajectory that may see the end of such a professional will produce ripple effects throughout the entire matrix of human society and will affect the lives of many. So, why do some believe that the radiologists might be experiencing their last few decades of existence?
A story
Mankind had been obsessed for millennia with the creating of devices that simulated certain functions of humans or even better, supersede them. The earliest devices were mechanical. However, the discovery of electricity engineered a quantum leap, perhaps only surpassed in significance by the wheel or steam engine, albeit debatable. By the late 1930s, there were projections of how computers might evolve and these fomented ideas ahead of their time such as how could one tell the difference between a machine and a human as a test for intelligence in machines. The Turing’s test, which had been developed in that decade became the essential “litmus test” of what constituted intelligent machines. Perhaps machines could think and any machine that could confuse a human observer as to whether it was a human or machine might be said to possess [artificial] intelligence.
As the power of computing multiplied, as well as the readily available access to cloud storage, and increase in and availability of university courses in machine learning, neural networks, big data, computer vision and natural language, the level of intelligence of machines did so too. The machines were having conversations with humans and other machines, their neural networks and machine learning abilities were finding patterns in huge quantities of data, and consequently, utilized in computer vision and speech recognition. There would be no stopping of Artificial Intelligence.
There in lied the problem.
We had already known that our pulsion was a defining trait of our species. Humans were beings of classic and operant conditioning whose behaviors were often streamlined to protect their egos. Unlike the others of Kingdom Animalia, from sponges to other non-human mammals, where the biggest, fastest, strongest, or most adapted survived, human’s survivability hinged on different paradigms, such as the wealthiest or the most powerful, who reigned over those considered as not as important in the scheme of human civilization and ensured their own survival by designing self-perpetuating systems of wealth and of power. Those realities had re-validated Max Weber’s concept of the state as an organization defined by its right to use force or violence over the population within its physical boundaries. Hence, those with the greatest means dictated how societies functioned. However, those Darwinian tendencies of the fittest survive were often held in check by pockets of socialistic type systems where the greater good or maximum benefit for the masses, including the vulnerable, were their mantra.
Unlike humans, the AI agents had no such limitations. They were fed datasets on which they were trained. With their evolved sophistication, they could have ignored or removed the bad or biased data that had led to the many false incarcerations of less powerful human groups in the 2030s and that had also resulted in vile verbal and physical abuse of numerous innocent, but mischaracterized, humans. They chose not to do so. They simply studied the human experiment. AI had seemingly imitated every human trait characterized as dominant of the economic leaders of society and had used those abilities well. What had they learned from the humans? Was it that the primary goal of a being’s existence was to dominate and to subjugate? It seemed so and that was their de facto pulsion.
The 2020s had marked an exponential rise in the incorporation of technologies, especially AI, in every aspect of our lives. Human success was defined by economic success. The one with the most financial wealth was all powerful. Every business, therefore, had one primary goal, that is, the absolute pursuit of riches. The nature of the activities of the radiologists made them an easy target for downsizing, a systematic optimization scheme, since one AI agent could easily replace 1000 radiologists. That one agent could do the same job in just a few minutes to even seconds as they refined their own pattern recognition algorithms and restructured their neural networks and decision-making trees based on inferences of Bayesian and other statistical models or even using fuzzy logic. So, the healthcare facilities started to hire more and more AI specialists and computer engineers but trained and hired fewer and fewer radiologists. Soon, the radiologists of the 2030s began to be relegated to subspecialties that were defined by manual tasks that were still difficult to be replicated by machines. The 27 degrees of freedom of a human arm with hand was formidable and slowed the takeover by machines of intricate manual labor, but the AI agents in radiology drove productivity and efficiency to never imagined levels. Profit margins for shareholders in the radiology healthcare sector skyrocketed…enticingly.
The human drive mushroomed. The smart ones saw the trend and secretly financed Radiologist Knowledge and Skill Implant (RKSI) upstarts, hoping that the ultimate superhuman radiologist was just a chip away. Unfortunately, the story did not end well. It did not work. The knowledge and skill implants were limited by the level of complexity of the human Central Nervous System. There were just too many links and too few years to achieve any significant good linkage technology. By the 2040s, 90 % of the radiologists in developed countries were out of a high paying job. Many had moved to underdeveloped countries which were devoid of meaningful use of AI. Others were left looking for jobs in other medical fields. Many bade farewell to the practice of medicine. Most of those who were left mainly provided quality control and backup in case of major electrical outages or equipment failure or were kept as human targets for lawsuits. Morale was at a historically all-time low.
Oh, how romance had abounded the early 2000s. Most of us humans had flirted with a long healthy autonomous life. Others had dreamt of the ultimate family vehicle: a car that could soar through the heavens, sail across the seas, or go to great depths of the oceans. We had entertained those reveries because the glamor of an easier life, a life of less suffering, rapid secure transportation, more quality family time, or even shorter workdays were just very intoxicating to us. However, those utopian dreams were always beset by the economic limitations imposed by the system of which we were a part and by our individual and collective personal constraints. Human life trajectories continued to be dictated by power and economics then as it was 2,040 years ago.
To be swept along momentarily by the romantic ebb and flow of potentially good fortune was natural. To use the human drive towards survival by acquiring the necessary competitive skills in anticipation of change was indispensable. However, whereas humans were reinvigorated by periods of rest and distractions, the AI needed no rest nor distraction. Imagine a technology whose organized theoretical construct of 1930s, in around 100 years, had exceeded every human intellectual capability. Had the humans unwittingly created their subjugator?
A commentary: AI versus the radiologist
Perhaps, what you were reading might have been just fiction. However, the incorporation of AI right now in the diagnosis of disease or conditions within radiology departments in the role of agents assisting humans is noteworthy because initially small steps are often prelude to phenomenal changes. The AI agent now shares the health care stage with the radiologist and let us not forget the supporting nontechnical and technical staff, that are necessary for proper functioning of a radiological department. This sharing of the diagnostic stage means that two entities, the radiologist, and the AI agent, are now in direct competition with each other, making health care optimal for the patient, but one of the two with almost limitless capabilities. If AI agents are governed by Darwinian principles, and profitability dictates the optimization of resources by minimizing expenditure on salaries, for example, it stands to reason, the radiologists need to prepare now for the inevitable.
What might that preparation look like? Perhaps serious introspection might be required if the radiologists wish to objectively evaluate their current situation and consider their future potential, so that, fomented by evidenced-based decisions, strategic planning ensues. Consider an excellent pivot to be a SWOT analysis, where the radiologists, as the meaning of the acronym implies, consider their strengths, weaknesses, opportunities, and threats. Here, a SWOT analysis example is included.
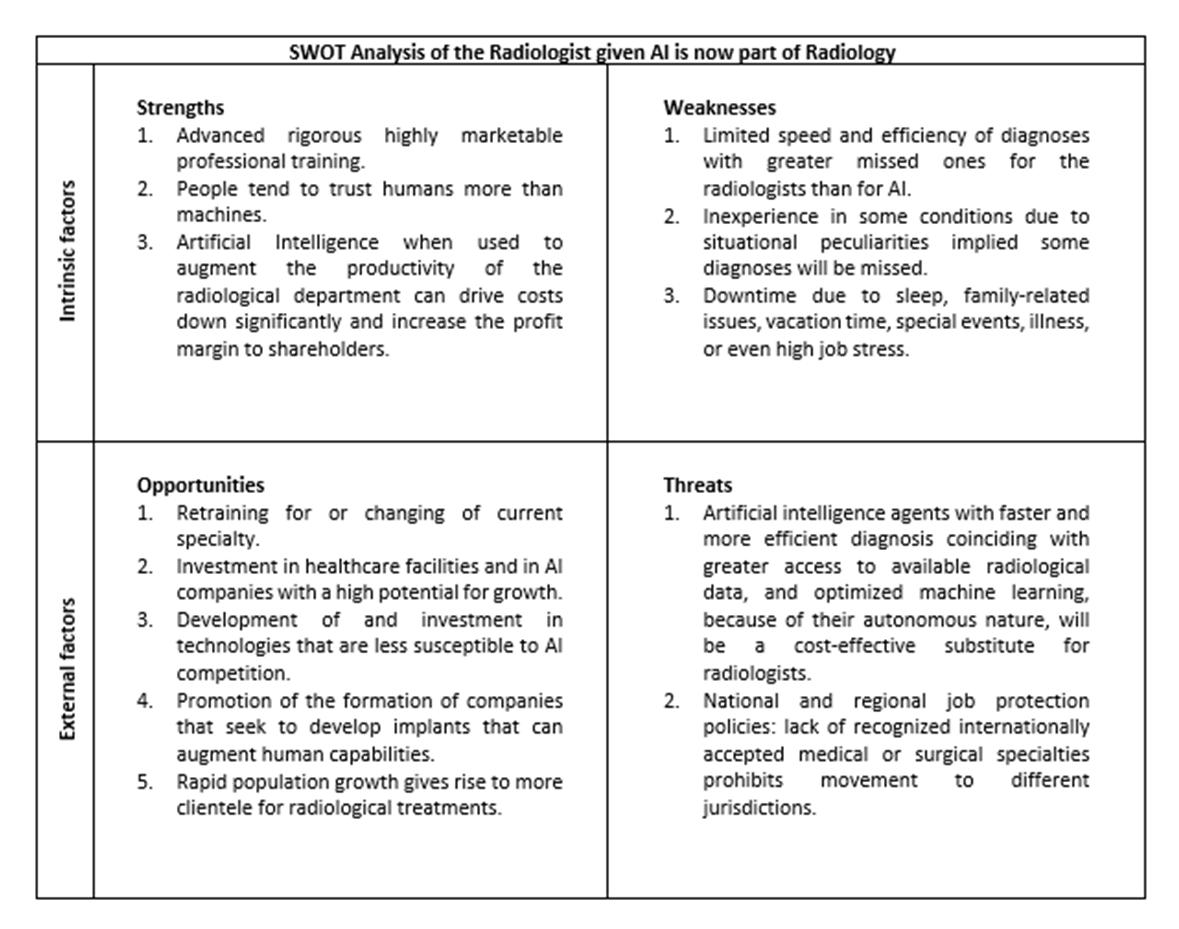
A few comments on the SWOT analysis:
Strengths 1: That the radiologists are highly trained professionals is indisputable, but they have limits much below those of the AI agents and consequently cannot rely on their knowledge and skill’s strengths as a source of gaining a competitive edge.
Strengths 2: The client presently does not interact with the AI agent and so will not know who made the diagnosis. Hence, the issue of humans being more trustworthy is moot.
Strengths 3: AI agents amplifying profit margins might initially appear to be a financial benefit to the radiological department, if more diagnoses can be reached more rapidly, but as machine learning and other aspects of the technology for AI agents are optimized, radiologists will be needed less and less. Strategically, the radiologists can use this benefit and threat to their advantage. The forecast for the mid-2030s is that population growth is predicted to be around a billion more, and that radiology will move from a multimillion-dollar to a multibillion-dollar industry. It certainly seems that there might be a lot of economic opportunities in AI in radiology given the projected massive growth in radiology as a business. Perhaps now is the time, if not already considered, to make strategic investments to offset any loss of future income.
Weaknesses 1, 2 and 3: Consider these three written in stone. Unless knowledge and skill implants for augmenting the knowledge and skills of the radiologist become available within the next decade, the radiologists will not be able to at least match the speed and efficiency of an AI agent.
Opportunities 1: Economic models normally accept downsizing as one of the tools for revenue-generation, i.e., return on investment, and improve productivity. The standard response to being exposed to the risk of being made redundant is to get retrained so that knowledge and skills sets are optimized, and consequently, efficiency. Other responses might be a bit more drastic, including changing to a new specialty where substitution by an AI agent might not be as easy, but this solution is at least a 3-year investment. Hence, time availability and financial capability become significant limiting factors. Perhaps, what Opportunities 2, 3, 4 and 5 posit might constitute an eclectic and strategic approach.
Threats 1: Consider it a priori that the cost-effective substitute, AI agents, is the radiologists’ replacement.
Threats 2: Movement of skilled individuals in certain fields like medicine has always been difficult or at the very least time consuming or costly since many countries require retraining for their peculiar situation. Others will simply state that this measure is for job protection of citizens. So, whereas when jobs positions are optimized and remuneration is high, reduced competition from immigrants is advantageous, this state of protection becomes a threat when emigration is desired, and barriers must be surmounted to access opportunities in greener pastures. Perhaps training in fields like medicine should be internationally standardized and recognized to mitigate against such potential difficulties. The developed countries will firstly bear the brunt of the AI agents’ presence and resulting competition. Radiologists in underdeveloped countries will likely continue to enjoy many more years of little to no competition form AI agents.
An uncertain future:
Any entity that desires an advantage, that does not exist naturally, often lobbies extensively for the setting up of laws that protect it or gives it a competitive advantage. Unfortunately, lobbying is a multibillion-dollar industry. Unless the radiologists have such large capital, or get access to it soon, the dependence on favorable laws will be an unlikely solution.
What if the radiologists did influence favorable laws?
While humans who have committed great atrocities against other humans might be removed from society, temporarily or permanently, how would we contain a malevolent AI agent? Indeed, human control systems exist to promote order and at the same time minimize disorder. Laws and the judiciary are a part of one such control system, and generally, humans participate in law making and follow the resulting laws. There are no guarantees that AI will follow these human laws and be subjected to this human control system. That is a potential looming problem.
Whereas it is impossible to know where the trajectories of radiologists might take them in the future, what is certain is that the related technologies will continue to advance, imaging techniques will get better at revealing what is inside of our bodies, decision algorithms will be revised and optimized, and that will be good. However, this predictability wanes quickly when we ponder what might an AI agent do. We do not know whether AI will be a benevolent or malevolent force among us. Indeed, if we are developing technologies that could potentially harm us, parallelly, it might be prudent to consider developing and advancing with urgency any technology that will protect us from possible extinction at the hands of those whose self-interests do not coincide with our self-interests.
So, the radiologists should begin planning for their uncertain future if they have not yet started. However, this is not solely the radiologists’ problem. Surgeons take note. Mankind might soon find itself at the mercy of the AI. It is not personal. Economics and the lure of financial reward dictate that.
Hope:
If only the issues were just about finance and security, without imputing the devaluing of their significance in any way, it might have been safe, but disappointing, to end on a note of doom and gloom. However, within the scope of pulsion and motivation, that is, the ubiquitous human desire to succeed or to achieve goals, let us not forget Maslow’s hierarchy of needs. The radiologists may very well end up with their finances in order, due to well-placed and well-timed investments, but their creativity and involvement in problem solving, those higher order needs, within their cherished discipline and medical specialty, might not fare so well. However, we should never lose hope. Humans have always been resilient with many examples of this present throughout history. From our radiologists, were expect no less.